FRCR Part 2B:
UK Trainee Insights
Pass rates for UK trainees sitting the FRCR 2B exam are decreasing. Our aim is to provide support on how to improve your chances of passing.
FRCR 2B Pass Rates: What the Data Shows
UK candidates have historically outperformed their global counterparts — but the trend is moving in the wrong direction. The January 2026 sitting, only the third under the reformed CR2B format, recorded the lowest pass rates in the available data. Part of this is attributable to the new exam format still finding its feet. But examiners have been unambiguous: underlying clinical and reporting weaknesses are a significant contributing factor.
Top 5 Mistakes UK Radiology Trainees Make in the FRCR 2B
The following were directly identified by examiners in the January 2026 sitting report. Notably, these are not new observations — the same patterns appear across multiple sittings.
-
Descriptive reports without a diagnosis Candidates describe findings but fail to commit to a diagnosis or differential. Simply noting increased opacification and recommending CT or MDT referral is not sufficient — examiners expect a clinical opinion based on patient demographics and history. Reporting
-
Insufficient pathological detail Vague descriptions such as "fractured radius" lose marks. The expected level is: "undisplaced, intra-articular fracture of the right radial head with associated joint effusion" or "Salter-Harris II physeal fracture of the left distal tibia." Reporting
-
Weak paediatric plain film interpretation Examiners specifically noted insecurity with paediatric cases and plain radiographic interpretation more broadly. Failure to recognise common cardiac devices on chest X-rays was flagged as a particular issue at this sitting. Clinical knowledge
-
Ignoring clinical context Not using the patient's age, sex, and clinical history to tailor differentials. A destructive bone lesion has a completely different aetiology in a child versus an adult — failure to account for this costs significant marks. Clinical knowledge
-
Poor exam preparation Candidates who did not practise on the risr/assess software platform before the exam were at an unnecessary disadvantage. The platform is not a PACS — image manipulation and scrolling take longer, and unfamiliarity costs time and composure. Exam technique
FRCR 2B Revision: What To Do After Passing the FRCR 2A
The breadth of the FRCR 2B oral exam is the thing that catches most candidates off guard. When I sat the exam — many years ago now — there were around 26 plain films across four vivas. Today, it is not uncommon for 60% of cases to be cross-sectional, spanning MRI head down to MRI feet. RCR data consistently shows candidates struggle most on nuclear medicine, mammography and ultrasound.
Work with colleagues to build a management database — pancreatic cysts, gallbladder polyps, BTS lung nodule guidance and so on. Much of this can be done in hospital hours. In your third year, attend different MDTs and make notes on how cases are handled. It does not need to be exhaustive — a couple per specialty is enough. If you can sit with radiologists during preparation time and note common management decisions, even better.
Pay particular attention to paediatrics. When you rotate through the paediatric block, make the most of it — ask for teaching on plain films and CXRs, and try to review the local case database. Do as much of this as possible in working hours.
How to Present a Case in the FRCR 2B Oral Exam
This is an issue for around 40% of candidates — but it is also one of the more fixable problems, and it responds quickly to the right kind of practice. Start six months before the exam. Study the gold standard answers below first, then work through the recommendations.
Case Examples
Below are two examples of how you should present cases in the oral exam.
Case 1: Chest Radiograph

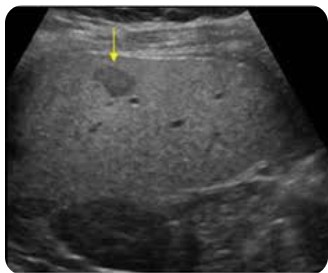
Case 2: Ultrasound — Incidental Liver Lesion
Every well-structured answer has five components. Miss any one of them and you leave marks on the table.
- Clinical history, clinical history, clinical history — This must be your first, second and third consideration when presented with a case.
- Articulate your findings. Speak clearly and systematically — what you see, what you don't see.
- Diagnosis. Use the history. If the patient has a cough and you see consolidation on a CXR it is likely an infection — say so.
- Differential — only if applicable. Not for the sake of it. Reticulonodular change in the lower lobes warrants a differential. A pneumonia in a young patient with a cough does not.
- Management. Keep it proportionate. A follow up CXR is sometimes all that is needed.
How to Improve Your FRCR 2B Oral Exam Technique
Write the five headings on a piece of paper and practise presenting on your own. Speak out loud and record yourself. Do ten cases per day — cases can be found on free teaching resources — and make sure all five headings are covered each time. The objective at this stage is simply to be a better you at case 50 than at case one. Be disciplined — do not neglect this step.
Repeat this now with a friend or ideally an FRCR 2B study buddy, taking turns to present cases to each other. Why? Because in the exam you will be presenting in front of others. You need to get used to it.
Think of the first 100 CT heads you reported — then the next 100. Everyone I have spoken to said they were faster, more coherent and less stressed on case 199 and 200 versus case 1 and 2. It will be the same here. The objective is to keep improving at this stage. You will not be ready just yet.
I would recommend at least 1,000 meaningful practice opportunities in your preparation. As time goes on you should aim to present a case in 60 to 90 seconds whilst following the recommended structure — 60 seconds for plain films and 90 seconds for cross-sectional cases. Cases can be obtained from books, courses and e-learning resources such as the oral section on this website. I do not know of anyone who has passed the exam without investing in some or all of these things.
Let me give you an example. A top FRCR candidate — now a very successful consultant — was asked in the oral exam whether microcalcification on a mammogram was anything to worry about. I will be honest, when this came up in the post-exam coffee session, yours truly drew a blank. The candidate had told the examiner it was not significant. At that point a breast-interested trainee interjected — to the collective horror of everyone gathered — that microcalcification is in fact a sign of potential malignancy and requires further assessment. Not one of us had known that.
Candidates with good exam technique can navigate many cases with examiner prompts, particularly cross-sectional imaging. However there are a few walls that even technically strong candidates hit — namely mammography, nuclear medicine and ultrasound. The reason, I believe, is that we tend to perform ultrasound in isolation with little opportunity to talk through what we are seeing. In contrast, we often encounter difficult CT and MRI cases in practice and can apply that experience in the exam.
Books, e-learning resources and courses have been designed to address this problem — it is worth asking peers what they recommend. Another useful strategy is to form a revision group and ask members to research guidelines and create crib sheets to share.
How We Can Help
We know the FRCR 2B can feel overwhelming — particularly when it comes to the topics that are hardest to get teaching on. Here is what we offer:
We offer revision lectures on the core topics candidates consistently struggle to revise independently.
An oral case database substantial enough to give you a solid grasp of presentation technique when used properly and consistently.
Targeted modules on the topics that are most difficult to obtain teaching on in clinical practice — the areas that catch even technically strong candidates out in the exam.
General FRCR 2B Revision Tips
The name of the game is to do as much as possible within your working day and protect your evenings and weekends. You will inevitably need to put in some time outside of hours — but every hour you invest at work is an hour you reclaim at home.
Most hospitals no longer have film viewing libraries, but Radiopaedia, Aunt Minnie and similar platforms are excellent alternatives. The principle is the same: share the load, revise together, and make the most of the people and resources around you.
In my experience, around 60% of UK candidates currently present cases to a good standard — similar to the style shown in Cases 1 and 2. Their technique is broad enough to handle the range of cases the exam throws at them, and they have found the right balance of presentation style, length and timing to engage effectively with the examiner.
But that figure has dropped. Five years ago I would have put it at 70%. And when I sat the exam myself — a long time ago — 70% of my cohort passed first time. The equivalent figure today is 45%.
I think COVID bears a significant part of the responsibility. It reshaped working patterns and made home PACS the norm. Before COVID, UK trainees benefited from years of consultant-led teaching in hospitals — the kind of informal, case-by-case instruction that is impossible to replicate at home. Many consultants now simply do not have the time to teach registrars in the way they once did.
Ultrasound is a particular casualty. It was once a consultant-led modality; now it is largely delivered by sonographers. The result is that many trainees arrive at the exam having had far less experience talking through ultrasound cases with a senior colleague — which is precisely what the oral exam asks of them.
Good luck with your revision.