FRCR 2B: Why International Candidates Fail The Oral Exam And How To Pass
Pass rates for the FRCR 2B are low and have been dropping over the decades. UK candidates fare better than international radiologists sitting the exam. Drawing on the experience of a consultant radiologist with over 15 years of teaching, alongside RCR examiners' reports, this article explores the scope of the problem and offers practical suggestions on how to improve your chances of passing.
Top 10 Mistakes International Candidates Make In The FRCR 2B Oral ExamInformation obtained from the RCR Official Examiners' Report
From The Teaching Room: A Real Case And What It Reveals
To try and understand what the official report says and gain an appreciation of where international candidates go wrong, please see a few real life examples of how international candidates who I have taught over the years approach a case.
Case 1: Chest Radiograph

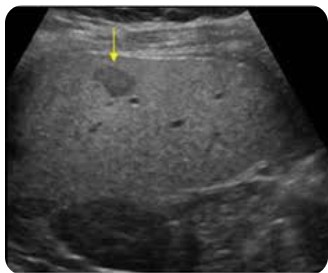
Case 2: Ultrasound — Incidental Liver Lesion
Having read both answers, ask yourself honestly — how close were you to the gold standard? In my experience only about 15% of international candidates can present close to this standard compared to 60% of UK trainees.
What Do We Recommend?
The breadth of topics that you might encounter makes this exam somewhat unpredictable — for example you might get a mammogram, DMSA scan, CXR and MRI liver all within the same six case packet. This is part and parcel of the oral exam but makes revision challenging.
Our key recommendations are:
- The purpose of oral exam preparation should be to develop a solid and reproducible technique that becomes second nature — one where you can speak without actively thinking, leaving you free to focus on diagnosis and management and interacting with the examiner both at the start and during the case itself
- Accept that you will be surprised. My experience is those candidates with a solid technique can navigate the unexpected.
From the gold standard answers above there are five components which are equally important and must be addressed to adequately navigate a case — the clinical history, your verbal presentation of the findings, what you think is going on, whether there are any differentials and finally what management is appropriate.
From My Experience Of Teaching, International Candidates Spend Around 70% Of Their Energy On Articulating Their Thoughts And Relegate Everything Else To The Background
- Clinical History, Clinical History, Clinical History — This must be your first, second and third considerations when presented with a case!
- Practise Articulating Your Findings. Recommendations 1 to 5 below explain how to develop your FRCR oral exam presenting style.
- Diagnosis. Use the history. If the patient has a cough and you see consolidation on a CXR it is likely to be an infection — say so.
- Differential Diagnosis — only if applicable. Not for the sake of it. Reticulonodular change in the lower lobes warrants a differential. A pneumonia in a young patient with a cough does not.
- Management. Keep it proportionate. A follow up CXR is sometimes all that is needed. Other times — "I am going to call the surgeon as the patient is obstructed and may perforate."
Write the five headings on a piece of paper and practise presenting on your own. Speak out loud and record yourself. Do ten cases per day — cases can be found on free teaching resources — and make sure all five headings are covered each time. The objective at this stage is simply to be a better you at case 50 than at case one. Be disciplined — do not neglect this step.
Repeat this now with a friend or ideally an FRCR 2B study buddy, taking turns to present cases to each other. Why? Because in the exam you will be presenting in front of others. You need to get used to it.
Think of the first 100 CT heads you reported — then the next 100. Everyone I have spoken to said they were faster, more coherent and less stressed on case 199 and 200 versus case 1 and 2. It will be the same here. The objective is to keep improving at this stage. You will not be ready just yet.
I would recommend at least 1,000 meaningful practice opportunities in your preparation. As time goes on you should aim to present a case in 60 to 90 seconds whilst following the recommended structure — 60 seconds for plain films and 90 seconds for cross sectional cases. Cases can be obtained from books, courses and e-learning resources such as the oral section on this website. I do not know of anyone who has passed the exam without investing in some or all of these things.
Let me give you an example. A top FRCR candidate — now a very successful consultant — was asked in the oral exam whether microcalcification on a mammogram was anything to worry about. I will be honest, when this came up in the post-exam coffee session, yours truly drew a blank. The candidate had told the examiner it was not significant. At that point a breast-interested trainee interjected — to the collective horror of everyone gathered — that microcalcification is in fact a sign of potential malignancy and requires further assessment. Not one of us had known that.
Candidates with good exam technique can navigate many cases with examiner prompts, particularly cross-sectional imaging. However there are a few walls that even technically strong candidates hit — namely mammography, nuclear medicine and ultrasound. The reason, I believe, is that we tend to perform ultrasound in isolation with little opportunity to talk through what we are seeing. In contrast, we often encounter difficult CT and MRI cases in practice and can apply that experience in the exam.
Books, e-learning resources and courses have been designed to address this problem — it is worth asking peers what they recommend. Another useful strategy is to form a revision group and ask members to research guidelines and create crib sheets to share.
How We Can Help
A lot of international FRCR candidates revise alone with time restrictions and struggle with exam technique. It is very easy to tell people to present concisely and quickly but the number of resources supporting this is low. The 200+ cases in our oral section are organised in a way that allows you to pick up the technique quickly. The e-lectures are something which have been well received. Our Nuclear Medicine, Mammography and Ultrasound modules allow you to revise the areas most commonly flagged in the examiners' report and practise your technique across different modalities.
If you are thinking of subscribing, maximum benefit is obtained after you have completed steps one to three in the recommendations above. If you already have some grasp of technique you will take considerably more from this resource.
If you have any questions please email us and we will do our best to help.
Thank you for reading this far. My parting word of wisdom is simple — do not give in to panic. I was an average trainee yet had no issues with the FRCR 2B exam. It is passable first time.